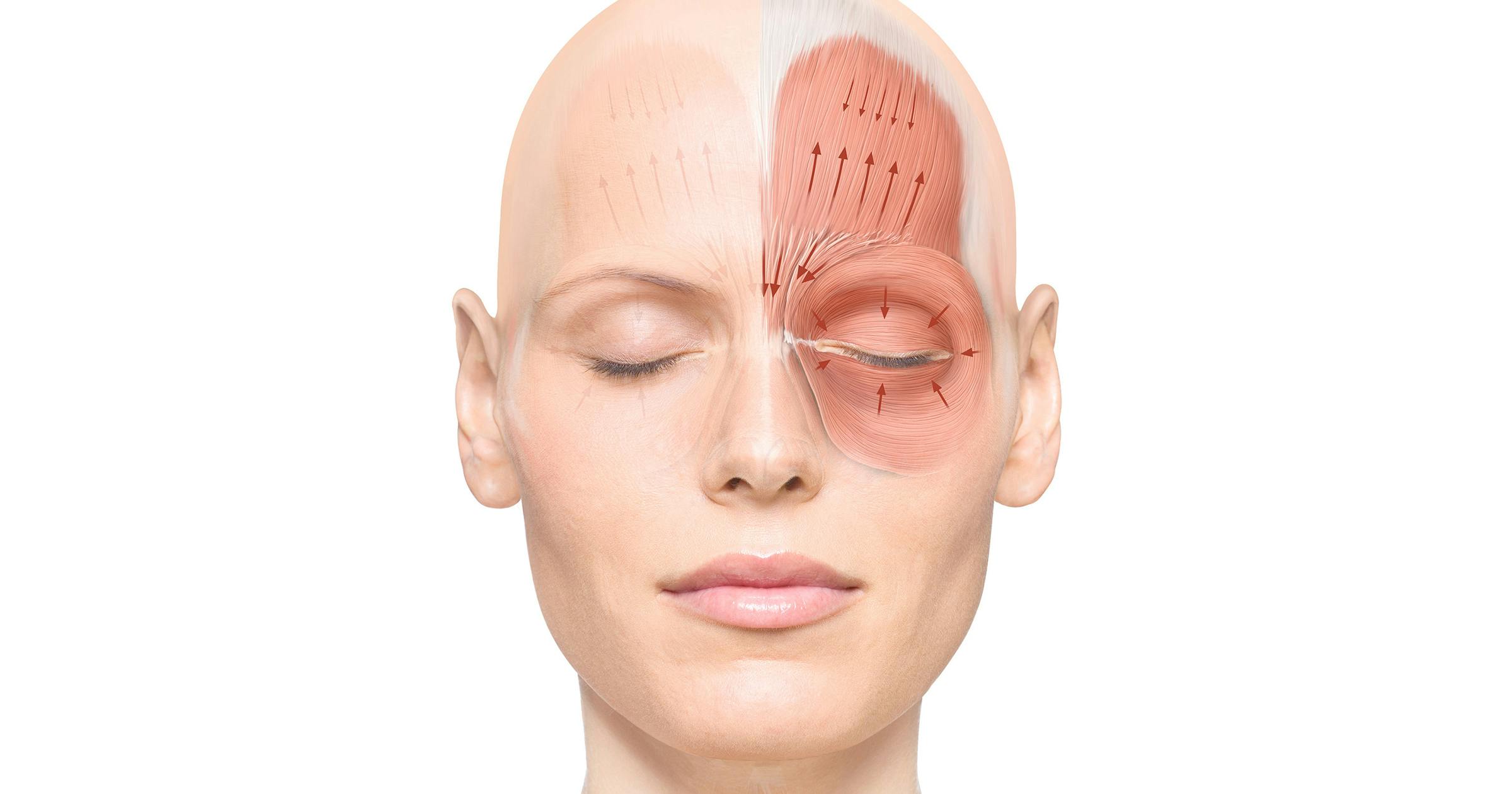
This indicates that despite the dislike of the overdone and overfilled facial appearances, aesthetic patients still favor a reduction of their facial rhytids to reduce the signs of facial aging. The most frequently requested facial regions to be treated with neuromodulators are the forehead, the glabella, and the lateral canthal region as these regions are often associated with an angry facial appearance. Interestingly enough, these facial regions are also those facial regions where the product manufacturers have their approved indications for the treatment with their approved products.
In the early days of neuromodulator treatments, the conducted injection algorithms focused predominantly on the skin surface appearance of facial rhytids.
Clinically, this meant that when a facial rhytid was visible the respective product was injected according to the clinical presentation of the rhytid. This went so far that in the late 2010s scientific publications were released that suggested to disregard the underlying anatomy and instead to inject according to skin wrinkle patterns. This resulted for instance in the unfortunate incorporation of glabellar contraction patterns into various injection algorithms when the area between the eyebrows had to be treated.

The glabellar contraction patterns suggested to deviate from the approved (by the regulatory boards of the respective countries) injection patterns and to instead simply look at the skin and to inject depending on how the skin was folding. Various publications followed from all over the world that expressed their confusion with these contraction patterns raising the need for a new standard when neuromodulators had to be injected.
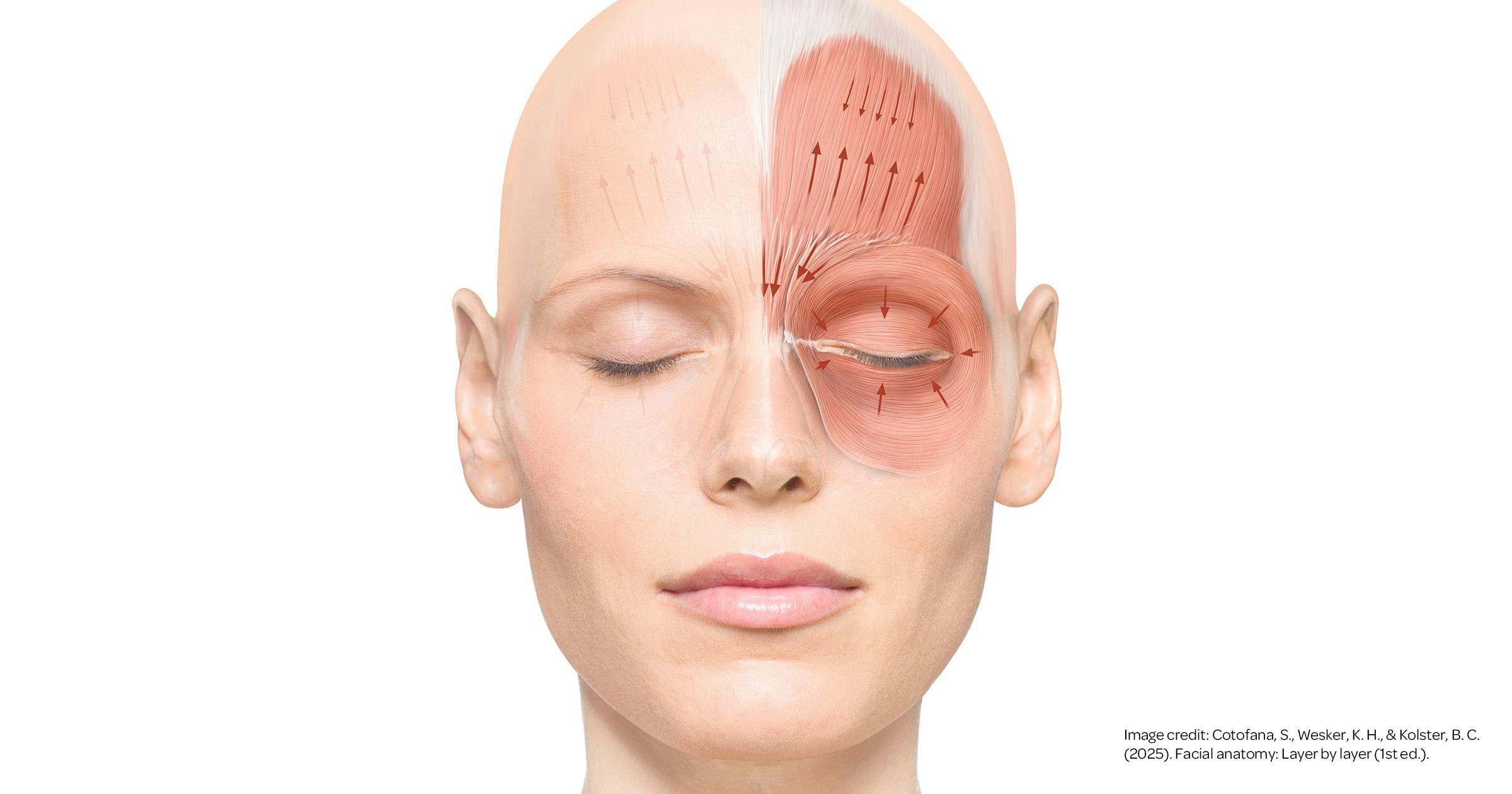
Magnetic resonance imaging-based studies and multiple clinical trials were conducted which revealed that the underlying muscular anatomy displayed no statistically significant differences in their muscle morphology when different glabellar contraction patterns were compared.
This implied clinically that every patient could and should be injected according to their underlying muscular anatomy and not based on the skin rhytid pattern with great and consistent clinical outcomes. When thinking about the mechanism of action of neuromodulators the above actually makes sense because toxins act at neuromuscular junctions where they temporarily block the release of acetylcholine containing vesicles at the presynaptic membrane; this prevents ultimately the signal transduction from nerve to muscle which results in a temporary muscle paralysis.
Therefore, the clinically correct injection algorithm for neuromodulator treatments should follow exclusively muscular anatomy and should not be influenced by skin surface phenomena.
However, in the past, the understanding of skin rhytid patterns and their incorporation into injection algorithms was still useful and should be respected. The ‘Gretchen question’ thereby is: HOW? How should skin rhytid patterns be included into neuromodulator injection algorithms? To find a solution to this problem the following past concept should be illustrated:
(Figure 1: Previous injection algorithms were based on the skin wrinkle pattern and less on the underlying anatomy.)
Instead of the past concept, which was partially disregarding the underlying muscular anatomy, it is proposed to adopt the new 3-step approach for neuromodulator treatments. This concept is currently performed worldwide by most injectors but it has not been proclaimed as the new gold standard nor has it been published in detail when addressing facial rhytids.
This 3-step approach is suggesting that the respective skin wrinkle pattern of any facial region is used to determine which muscle or which muscle group is responsible for the formation of those specific wrinkles. A clear anatomic understanding of the underlying musculature is therefore needed which includes the function of the muscle, its origin, its insertion, and the distribution of the neuromuscular junctions within the muscular tissue.
Once the “culprit” muscle has been identified the skin wrinkle pattern needs to be disregarded and only the knowledge of the underlying muscular anatomy should be used as guidance for the toxin treatment. This might be counter intuitive because one would assume that the underlying musculature would be directly or in some dedicated ways be connected to the wrinkle pattern of the overlying skin. However recent research has indicated otherwise and has failed to establish correlations between skin wrinkle pattern and muscular anatomy.
Clinically, this means that only the underlying musculature is responsible for the skin rhytid pattern and not the skin or the soft tissue itself; the latter are anyway not amenable to the neuromodulator product. Therefore, the new 3-step approach would look as follows:
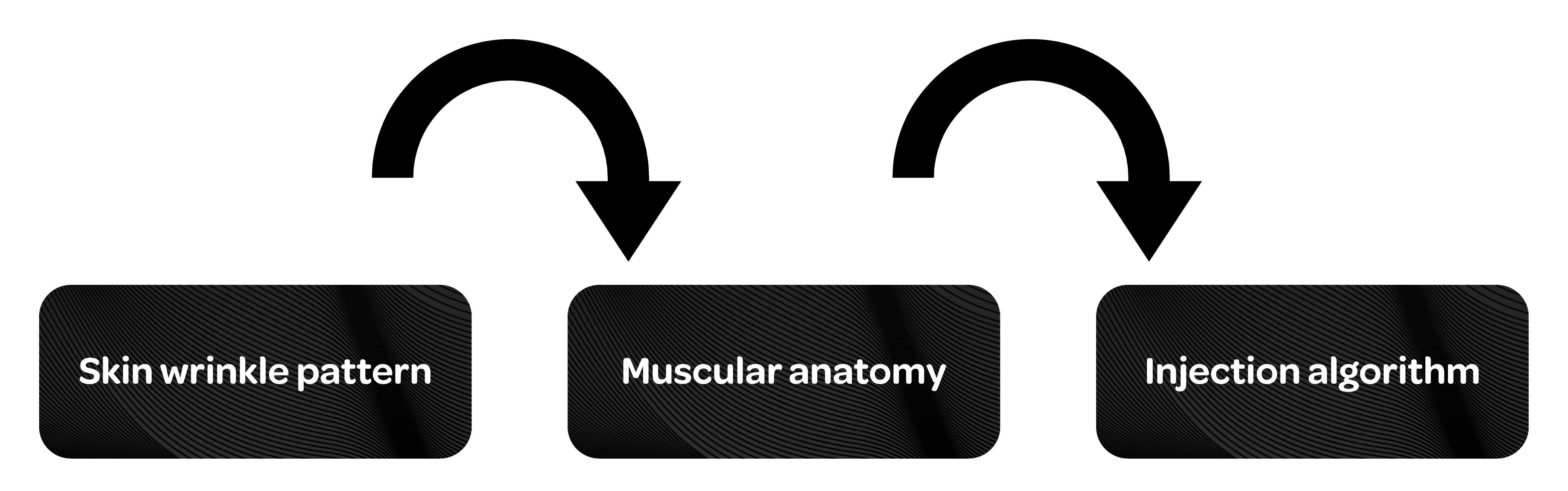
(Figure 2: The 3-step approach for neuromodulator treatments)
The above illustration shows that when determining which injection algorithm is needed to address the aesthetic needs of the patient, the underlying muscular anatomy should be the driving factor and not the skin rhytid pattern; the latter however can be used to identify which muscle or muscle groups are involved and need treatment.
The above depicted 3-step approach might sound familiar and plausible; and yes, it is! But looking back at the early days of toxin treatments, an outdated, non-anatomic approach was performed which resulted in suboptimal outcomes with business- and reputation-damaging clinical results.
It is hoped that the new 3-step approach will help to guide injectors toward safer, more reproducible, and longer-lasting clinical outcomes.
Because at the end of the day, it is all about clinically applied anatomy.
Join our community for news, offers, and updates on Cotofana Anatomy’s events and resources
Copyright © 2026, Cotofana Anatomy. All rights reserved.

