The concept of the Line of Convergence, also referred to as the C-Line, has been present in humans for a very long time. However, it wasn’t until 2020 that a group of researchers found the correct methodology to measure and quantify it.
This is a very important statement to make at this point because it sets things into perspective: just because something is not published or validated by the laws of science does not mean it did not exist prior to that.
For the Line of Convergence, the same concept applies; it existed long before my research group described it.
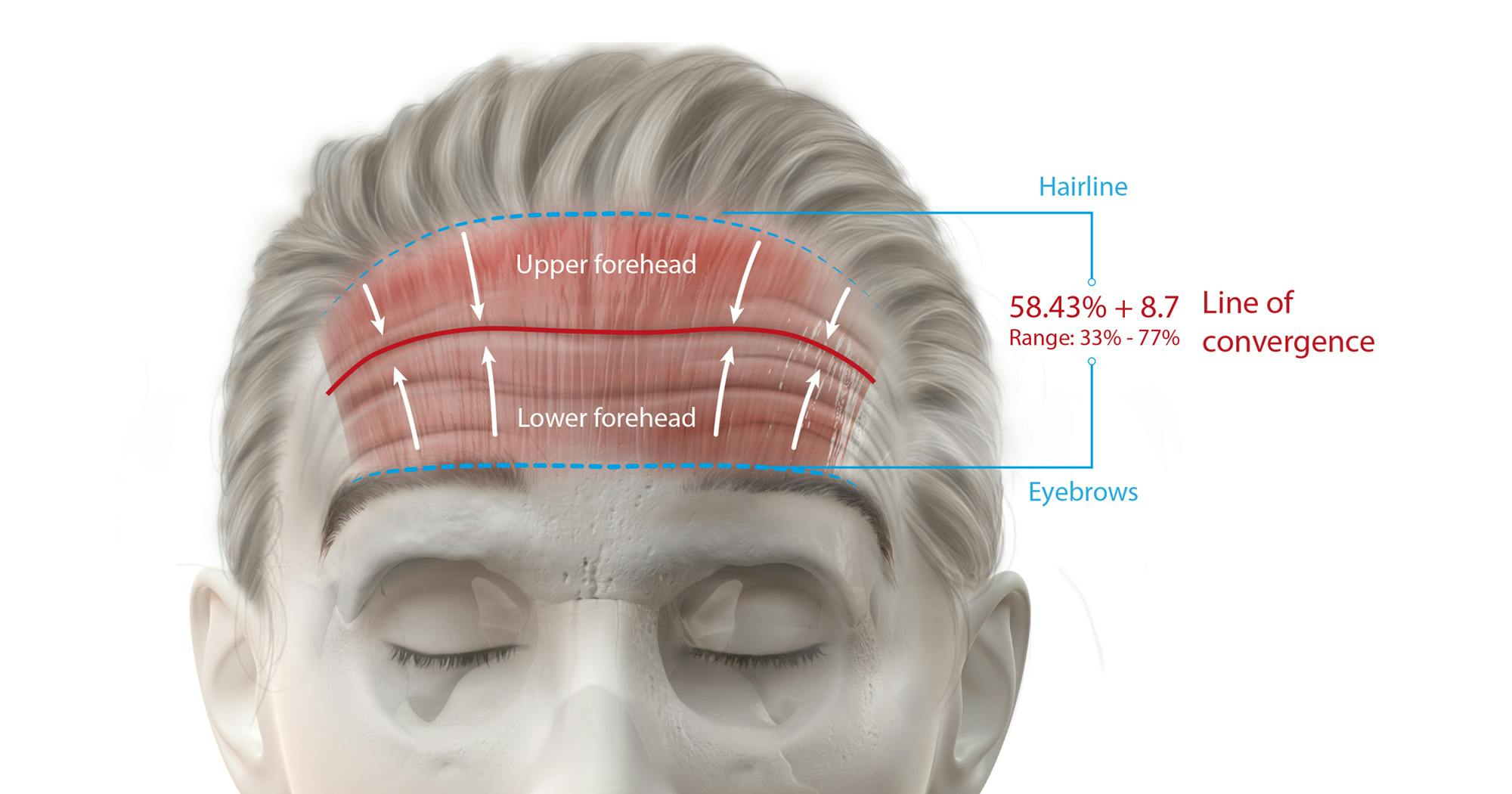
The Line of Convergence concept is used world-wide to guide neuromodulator injections for the treatment of horizontal forehead lines. This skin surface landmark is located on average at 60% of total forehead length when measured as the distance between eyebrows and hairline and separates the frontalis muscle in two portions: the frontalis muscle below the Line of Convergence is regarded as an eyebrow elevator, whereas the portion of the frontalis muscle above the Line of Convergence is regarded as a hairline depressor.
This separation of the frontalis muscle in two different functional units can guide and improve neuromodulator treatments. Injections at and above this line can be administered deep or in larger quantities and will not have a major impact on the position of the eyebrows, because this part of the muscle is not responsible for eyebrow positioning. Whereas injections below this line need to be administered superficially or in reduced quantities in order to avoid eyebrow ptosis.
The latter arises from the relaxation of the eyebrow elevation segment of the frontalis muscle which – when relaxed - is unable to elevate or suspend the eyebrows causing a drop in their position.
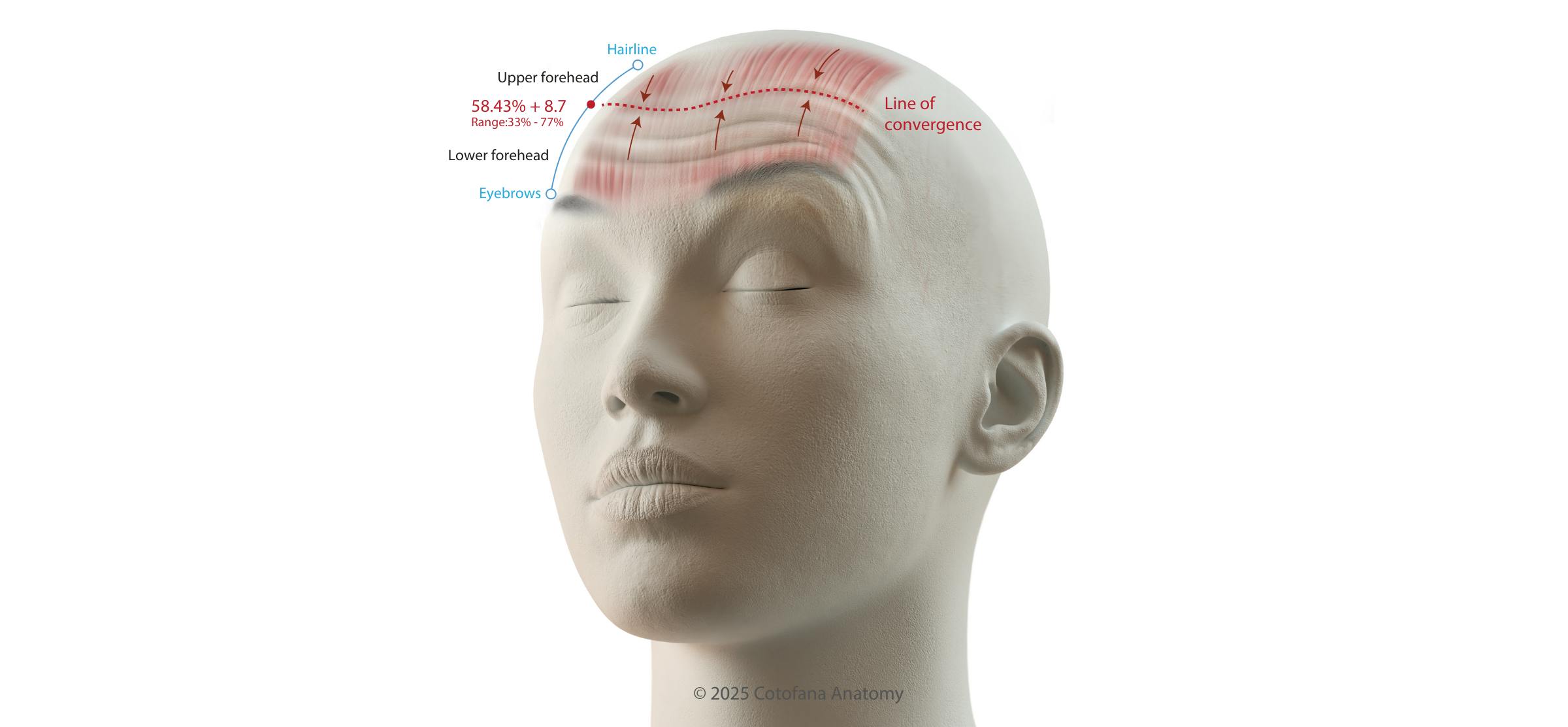
There are several ways to identify the location of the Line of Convergence in the forehead. The reason why this is so relevant is because the C-Line can be located somewhere in the forehead ranging between 33 - 77% of total forehead length. This indicates that there is anatomic variation and therefore individualized treatments require the accurate identification of this skin surface landmark:
Some authors have described that the line of convergence does not exist or is hard to find in some patients. Others have even come up with AI-based assumptions which state that the frontalis moves only in one direction and does not have a bi-directional movement… despite multiple independent studies having confirmed its presence in various clinical and basic science investigations.
To provide clarity on this topic and to explain why in some patients the C-Line is not so easy to identify let’s go back… very far back… into the basics of muscle histology and physiology and revisit the fundamentals of a muscle’s contraction.
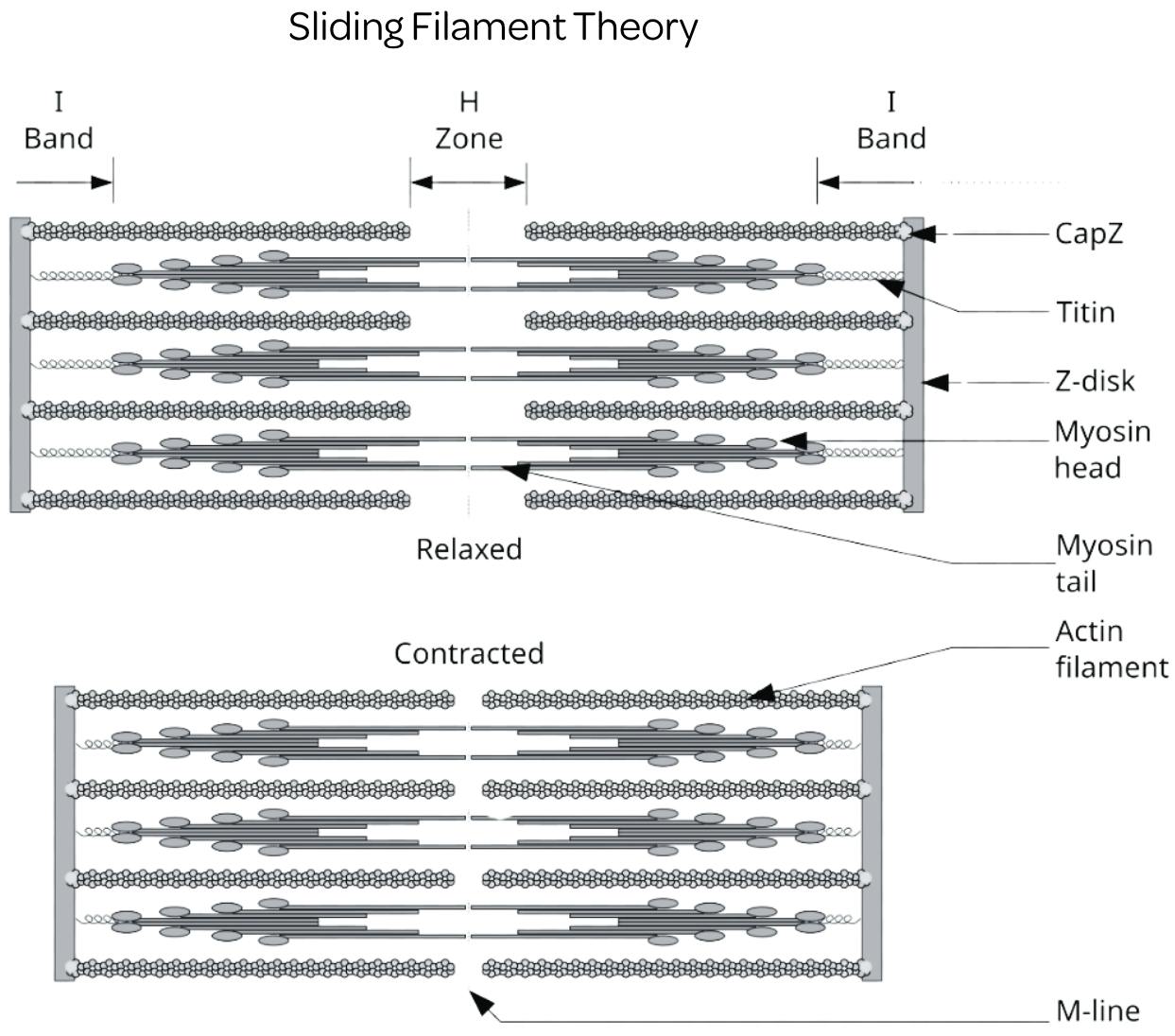
The current understanding of a muscle’s contraction is based on the Sliding-Filament-Theory, which was first published in 1954 both (but independent of each other) by Andrew Huxley & Rolf Niedergerke and by Hugh Huxley & Jean Hanson. Via microscopy and X-ray diffraction, they discovered that tubular shaped proteins called myofibrils (the most prominent are called actin and myosin) inside muscle cells do not shorten but glide past each other thereby shortening the subunits of a myofibril which are called the sarcomeres.
This sliding mechanism allowed for the approach of both ends of a sarcomere called the Z-discs (or Z-band) toward each other collectively resulting in the overall shortening of a muscle cell. Because the thick filaments called myosin were anchored to the muscle cell membrane, the only possible movement is toward the center of the myofibril, respectively. One can imagine that when all sarcomeres within a myofibril shorten toward the center of the sarcomere, the overall contraction of a muscle is bi-directional.
Normally, one part of the muscle is attached to a bone (which is called origin) whereas the other part of the muscle is connected to another bone (which is called insertion). Which bone is moved during muscular contraction depends on which of the two bones is fixed to the core of the body or to other stabilizing structures. Imagine now that none of a muscles’ origin or insertion is fixed and both ends can freely move, as is the case for the frontalis muscle in the forehead. Then, the resulting movement is a bidirectional movement toward the center of the muscle in which the origin approaches the insertion.
And this is exactly what can be observed clinically in the forehead: eyebrows approach the hairline and both movements converge toward an immobile region: the Line of Convergence. But given that there is anatomic variation for the frontalis muscle like it is for the presence of a central tendinous aponeurosis or like it is for its connection to the occipitalis muscle (the true and correct name for the frontalis muscle is: anterior belly of the occipito-frontalis muscle; also referred to epicranius muscle) we can all imagine that the Line of Convergence is subject to anatomic variation. On average it is located at 60% of the total forehead length but keep in mind that the frontalis muscle can extend past the hairline and its strength can vary. Therefore, individualized assessment of the Line of Convergence is needed when targeting horizontal forehead lines with neuromodulators.
Join our community for news, offers, and updates on Cotofana Anatomy’s events and resources
Copyright © 2026, Cotofana Anatomy. All rights reserved.

