In the beginning of soft tissue filler injections, the belief was that once a product in injected into the face, it will stay in its targeted location and will not move anywhere else: deep supraperiosteal injections will result in product deposition that is overlying the bone (and nowhere else). Similarly, if the subdermal plane was targeted, the product would stay in the layer below the skin (and nowhere else).
However, research studies as early as 2019, started to reveal that product migration exists, and that soft tissue filler product moves into various other 2-dimensional and 3-dimensional locations. The migration or spread happens either directly during the injection process or in the period afterwards. This resulted in the understanding that various factors need to be considered which are capable to ultimately influence where a product will reside in the end.
The knowledge about such factors and the research field investigating those factors was termed Injection Biomechanics. Multiple research studies revealed remarkably interesting facts. The following factors influence product distribution/migration:
Interestingly, the underlying layered anatomy was not identified to be an influencing factor as multiple independent studies have shown that the laws of injection biomechanics apply for every region of the human body and not only for the face or parts of the face.
Focusing on the face, however, the currently most accepted anatomic concept to describe the fascial layers is the concept of the 5 layers of the face. These 5 layers are parallel to the skin surface and indicate the existence of a superficial and of a deep fatty layer. This concept is exemplified in the below AI generated image.

Figure 1: The 5 Layers of the Face concept, exemplified on a full-thickness tissue block.
When comparing Figure 1 to a real ultrasound image that was taken from the cheeks (of an aesthetic patient) big differences can be observed. The most striking difference is that no clear separation exists between the fascial layers as shown in Figure 1 and that the superficial and the deep fatty layers are not homogeneous within themselves but instead highly structured and continuous with each other.

Figure 2: Ultrasound image of the cheeks in horizontal orientation. With permission from Dr. Leonie Schelke.
This ultrasound image does not correspond to the current concept of the layered arrangement of the face (as shown in Figure 1), and it seems that theory is far away from reality in this case. To make things even worse, I conducted a cryosection of the cheek region back in 2015 and have found upon review of these old datasets interesting similarities between the ultrasound image (of a living patient) and of a human body donor as shown in Figure 3 below.

Figure 3: Cryosection of the cheek region in view from inferior. The big dark red structure is the temporalis muscle located inside the temporal fossa and it is overlayed by the various (more than 5) fascial layers.
Both the cryosection (Figure 3) and the real-time ultrasound of the cheek (Figure 2) show that no clear separation exists between the various fatty layers but instead they all seem connected with each other. In addition, it seems that there are multiple fascial layers present and not only a superficial and a deep fatty layer. Distinct and detailed fat compartments with strong compartmental boundaries seem to not be present but instead a highly structured and organized 3-dimensional connective tissue network that spans from the deep layers to the dermal undersurface and envelopes the various fat lobules.
If the concept of the 2 fatty layers (superficial and deep) does not exist but instead a continuous 3-dimensional network of fat and fascia which allows for multiple interconnections, it would explain plenty of clinical observations including the product diffusion/spread phenomenon between deep and superficial fascial layers during soft tissue filler injections.

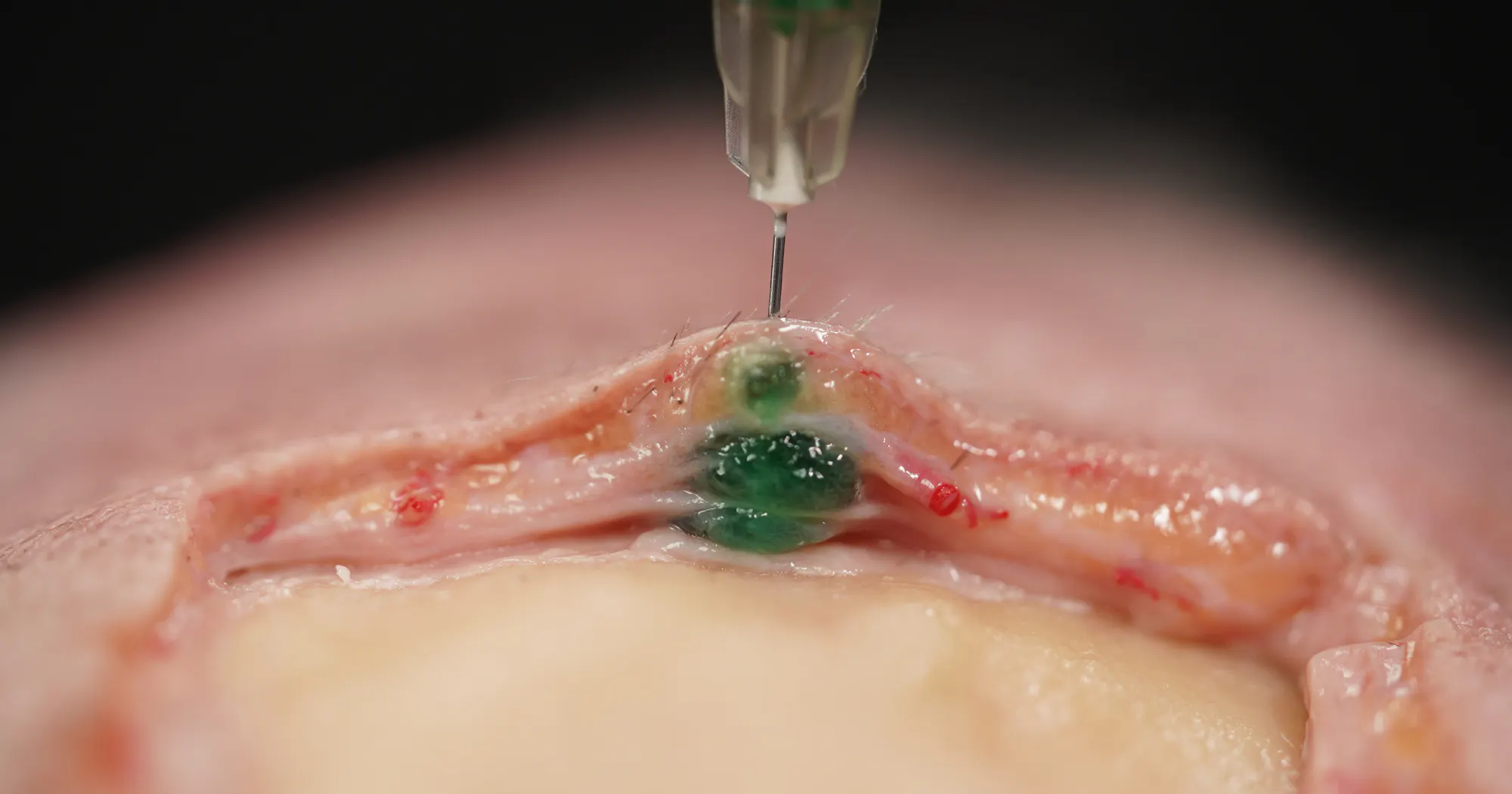
Figure 4: Green dye injection into the cheek region of a human body donor.
Looking with detail at the green dye injection which I performed with a needle in perpendicular and constant bone contact reveals that the product does not stay in the deep plane alone but moves upwards along the created injection canal until reaching the dermal undersurface. This phenomenon has been confirmed in various research studies as well in daily clinical practice. This product diffusion can be explained by the 3-dimensional connective tissue architecture which allows for interconnections between fascial planes and fatty layers and which must be considered rather a loose than a strong barrier.
All of the above facts seem to point into one direction which is currently only speculation: the concept of distinct and strongly bounded fat compartments and fatty layers seems to be outdated and a new concept needs to be identified. A concept that incorporates clinical findings, ultrasound imaging, alongside a strong and modern anatomic support. A concept that goes along with clinical observations, but which is based on anatomy.
Many new provocative thoughts may be stirred with this article but the way into the future is only together: clinical observations and basic science. Only together, the intricacies of nature can be revealed.
Join our community for news, offers, and updates on Cotofana Anatomy’s events and resources
Copyright © 2026, Cotofana Anatomy. All rights reserved.

